Arthritis of the knee refers to damage to the smooth cartilage which normally lines the end of the bones. This can be caused by wear and tear, as a result of a previous injury, or can come on for no obvious reason. It sometimes runs in families. It typically affects people in their 60s and 70s, but not uncommonly affects younger adults. When the cartilage wears down to bare bone the condition becomes serious.
The knee has three different compartments, the medial (inner), the lateral (outer), and the patello-femoral (under the kneecap) compartments. Arthritis can affect an individual compartment, or a combination of the two. Most commonly arthritis affects the medial, or inner, compartment of the knee.
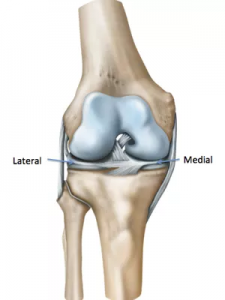
Diagram of the knee from the front
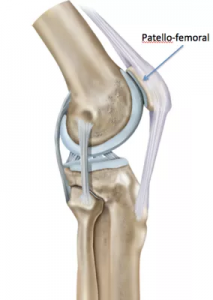
Diagram of the knee from the side
You will experience pain in the knee. To start with this is worse with activities, typically walking. You may also notice stiffness and swelling in the knee. Kneeling down may become difficult. It may be uncomfortable to sit for prolonged periods, and stiff when you first get moving again. The pain is typically a dull aching pain somewhat like a tooth ache. In the early stages it will respond well to anti-inflammatories or painkillers, but as the condition progresses these become less effective.
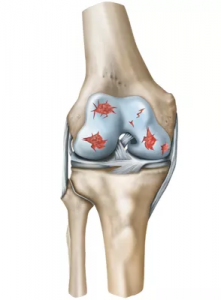
Diagram of an arthritic knee
In the early stages of arthritis painkillers, physiotherapy, and walking aids such as sticks can be helpful. As the condition progresses injections of steroid or replacement joint fluid (Durolane) can be useful. Previously keyhole (arthroscopy) surgery was used for early arthritis to ‘wash the knee out’, but good scientific studies have shown that for simple arthritis this is not very effective. However if there are symptoms coming from a torn meniscus, or loose pieces in the knee then arthroscopic surgery is still very useful.
With time this will affect your mobility, and you’re walking distances. It will impact on your lifestyle, and impair quality of life. It may become painful at night-time and keep you awake at night or wake you up from sleep. When the symptoms reach this level it is time to consider having surgery in the form of a knee replacement.
The knee replacements that we use today are very sophisticated pieces of metal and plastic. However they still have a finite lifespan. For this reason, the younger you are when you had a knee replacement the more likely it is to wear out in your life time. For that reason we try to avoid knee replacement surgery in young patients where possible.

Total knee replacement
Depending on the pattern of your arthritis, and the compartments of the knee involved you may be suitable for surgery to realign the leg (osteotomy) or partial knee replacement (uni compartmental knee replacement \ Oxford knee replacement). For total knee replacement modern technology allows us to make instruments specific to your knee based on scans (patient specific instruments). This allows very precise positioning of the new knee in order to give it the longest possible lifespan and best possible function for your new knee.
If you think you have knee arthritis it is well worth getting it checked out by Dr. Amit sooner rather than later. He has considerable experience in all techniques regarding knee arthritis and offers the very latest techniques in knee replacement surgery.